Integrated Neighbourhood Teams, Fuller approach, Integrated Care
Dr Claire Fuller, General Practitioner — and at the time of writing the Fuller Stocktake CEO (designate) of Surrey Heartlands ICS — proposed the building of integrated teams in every neighbourhood of 30-50,000 people.
In this model, teams from across primary care, community care, secondary care, social care, the voluntary sector and others would work together in multidisciplinary teams delivering care, improving health and tackling health inequalities in their neighbourhood.
There was an explicit recognition that people have historically worked in siloes and an implicit suggestion that creating these neighbourhood teams would create more “joined-up” care for people and patients, something that has been a goal for the NHS for many years.
The Fuller approach to integrated care
So what is new, and for me promising, about the Fuller approach to integrated care?
- A team of teams, not a single team for everything
- Not a new organisational form
- Teams at the “neighbourhood level which make sense to local professionals and local people
- Teams with a focus
With a refreshing focus on the different types of care needs, this nuanced vision has a real chance of success if properly implemented.
Claire proposed three main types of need:
- People who are generally well but get an acute illness – what we would call “urgent care” or “same day demand”
- Proactive, personalised care for people with complex needs
- Preventative care
Building a fuller picture of integrated neighbourhood care
In addition to the needs outlined in the Fuller Stocktake, I would add:
- Reactive care for people with complex needs who deteriorate
- Long-term condition management
This means four (people with complex needs require a single proactive AND reactive care model) micro-teams within a big neighbourhood team.
Each micro-team would have its own focus, functions and roles. Each team would be perfectly formed to meets its focus, objectives and outcomes. Each micro-team would be part of a wider whole.
I have illustrated this in the matrix below:
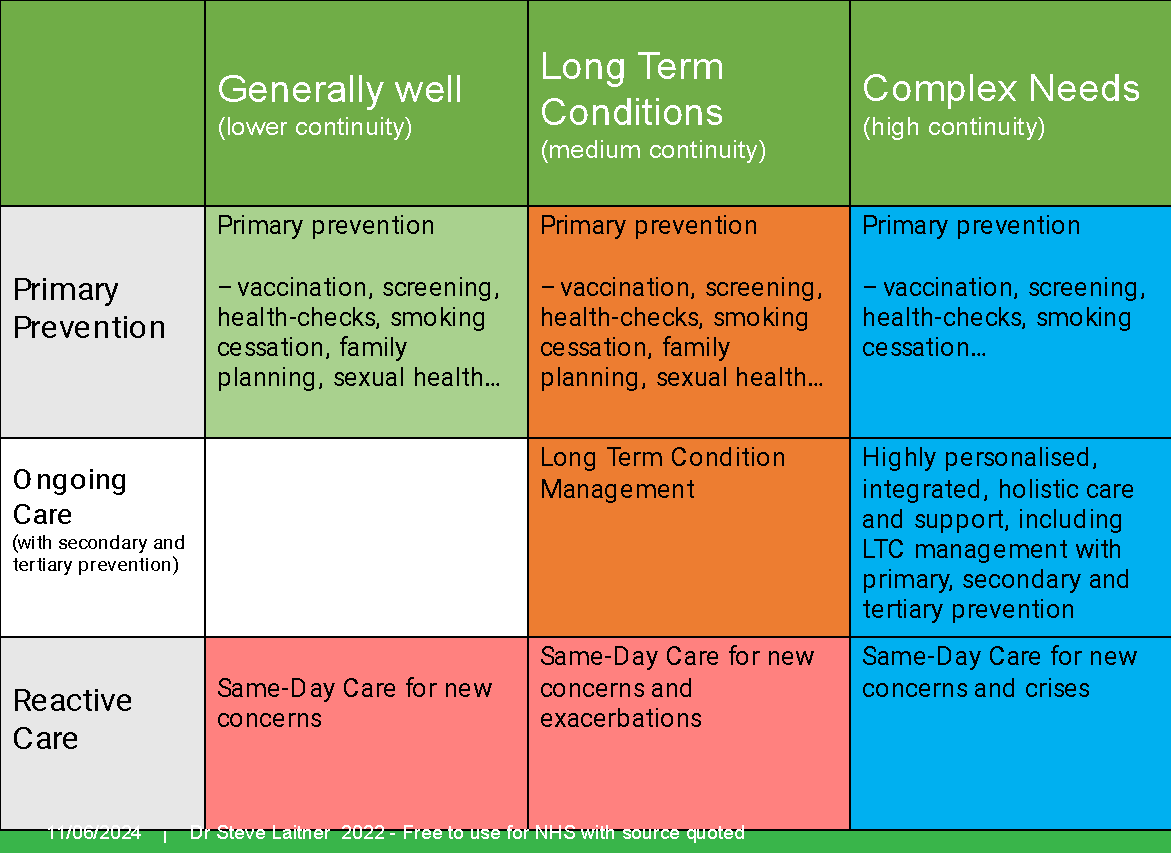
So we have:
- A prevention team
- An acute care team
- An LTC team
- A complex needs team
It might be the case that some of these teams sit better at a practice level, some at a PCN level and some at a place level. This can be determined locally and evolve.
Focusing on differing patient and staff needs at scale
What matters is the recognition that health and care, of all the types above, is a team sport and that different groups of people have different needs (and preferences). Naturally, they require different approaches, functions, skills and people involved.
It means that everyone doesn’t have to do everything. Staff can do more of what they like and what they are good at while still moving between teams for training, experience or because they want variety.
From Plato to Adam Smith we have known that division of labour is a good thing for society. We also know that people work well in teams with a shared vision and focus.
We also know that a sense of place/ community is important for people, both at work as well as at home.
Filling in the missing pieces with population health management
The missing part of the jigsaw in my mind has been a more nuanced sense of population needs in a segmented way — something we now call Population Health Management.
I thank Claire for finally bringing a sense of nuance to primary care, making Population Health Management a reality and giving us a clear direction of travel.
Now is the time to move on from a one size fits all approach to primary care.
Bring on the micro-teams!
Getting started with Integrated Neighbourhood Teams
Ok, but what do we actually do? Where do we start?
My advice: don’t start with the team. And certainly don’t start thinking of a new statutory organisational form. Team members can leave their organisational name badges at home. For example, someone can say “ I work for the St Albans and Harpenden Frailty Team” rather than I work for “Hertfordshire Community Trust”.
So start with the problem you most want to fix — same day demand, prevention in those who are currently well, long term condition management or people with complex needs.
Then, think about the care needs (and preferences) of that group of people with those needs.
What care functions do you need (such as care coordination, comprehensive geriatric assessment, care and support planning, medication review, clinical triage etc)? Then build your micro-team and start caring!
Then move on to your next priority. After a while, you’ll have your ‘team of teams”.
It will be a long journey of continuous improvement, but you won’t be on your own.
Steven Laitner is a salaried GP in St Albans, Hertfordshire. He has a public health and clinical leadership background and supports healthcare organisations with population health management and service redesign.
@SteveLaitner

